What is New York’s Medical Aid in Dying Act – and How Will it Work?
After nearly a decade of legislative debate, New York is set to join a growing number of states that permit medical aid in dying (commonly referred to as assisted suicide) for terminally ill adults. On December 17, 2025, Governor Kathy Hochul announced that she reached an agreement with legislative leaders to move forward with the Medical Aid in Dying Act, confirming that she will sign the bill in January 2026, with the law taking effect six months later to allow time for physician training and regulatory guidance.¹
This article is intended to provide a neutral, factual overview of the law’s history, its final structure, how New York’s approach compares to other states, potential concerns raised by advocates, and what this development means for estate planning and advance care discussions.
A Long Legislative History: What took so long?

New York’s Medical Aid in Dying legislation was first introduced in 2015, shortly after similar laws were enacted in states such as Oregon and Washington.² Over the next ten years, the bill was introduced and debated multiple times but failed to advance due to a combination of factors, including:
Ethical and religious objections,
Concerns raised by disability-rights advocates,
Fears of coercion or pressure on vulnerable individuals, and
Disagreement over what safeguards should be required.³
Although public opinion in New York gradually shifted and more states enacted similar laws, consensus remained elusive. In 2025, the bill finally passed both the State Assembly and Senate. Governor Hochul then delayed signing while negotiating additional protections, ultimately announcing in December 2025 that she would approve the legislation with added guardrails.¹
What the Original Bill Allows
Under the framework passed by the Legislature, medical aid in dying allows a mentally competent adult with a terminal illness and a prognosis of six months or less to request medication that they may choose to self-administer to bring about death.⁴
Key elements of the original bill include:
The request must be made directly by the patient; it cannot be made by a health care proxy, agent, or family member.⁴
The patient must make both an oral request and a written request.⁴
Two physicians must independently confirm eligibility, diagnosis, prognosis, decision-making capacity, and voluntariness.⁴
The patient must be informed of alternatives, including hospice and palliative care.⁴
The patient may rescind the request at any time.⁴
Health-care providers may decline to participate and are protected from liability when acting in good faith.⁴
This structure mirrors the general approach taken by many other states that allow medical aid in dying.
Governor Hochul’s Added Guardrails (as of December 2025)
Before agreeing to sign the law, Governor Hochul required several additional safeguards, which are now part of the final version of the statute.¹⁵ These include:
Mandatory mental health evaluation
Every patient must be evaluated by a psychologist or psychiatrist to confirm capacity and lack of coercion.¹
Recorded oral request
The patient’s oral request must be documented by audio or video recording.¹In-person initial evaluation
The first physician evaluation must take place in person, rather than exclusively via telehealth.¹Waiting period
A five-day waiting period is required between when the prescription is written and when it may be filled.¹Witness and interpreter restrictions
Anyone who may financially benefit from the patient’s death may not serve as a witness or interpreter.¹Residency requirement
Eligibility is limited to New York residents.¹Professional misconduct enforcement
Violations of the law constitute professional misconduct under state licensing laws.¹Delayed implementation
The law will take effect six months after signing, allowing time for regulations, training, and guidance.¹
The stated purpose of these guardrails is to increase oversight, protect vulnerable individuals, and ensure consistent implementation statewide.¹
How New York Compares to Other States
As of late 2025, **medical aid in dying is authorized in 12 states and Washington, D.C.**⁶ These jurisdictions are:
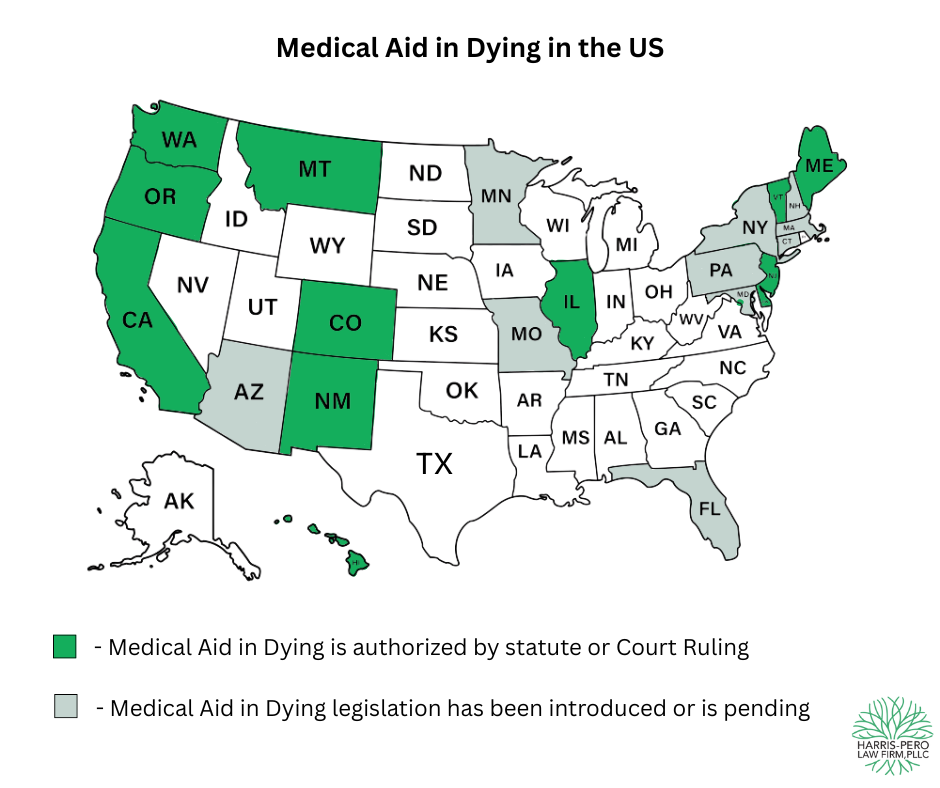
**California, Colorado, Delaware, Hawai‘i, Illinois, Maine, Montana (by court ruling), New Jersey, New Mexico, Oregon, Vermont, Washington, and Washington, D.C.**⁶
The following states have introduced medical aid in dying legislation or are anticipated to enact such laws in 2026:
** Arizona, Connecticut, Florida, Illinois, Maryland, Massachusetts, Minnesota, Missouri, Pennsylvania, and New Hampshire**
Common Features Across States
Most medical aid in dying laws share several core requirements:
A terminal illness with a six-month prognosis,
Patient-initiated requests,
Confirmation of decision-making capacity and voluntariness,
Review by at least two clinicians, and
Self-administration by the patient.⁶
Where New York Is More Restrictive
Compared to many states, New York’s law includes safeguards that are more stringent than the national baseline, including:
A mandatory mental health evaluation in every case, rather than only when capacity is in doubt,
A requirement that the oral request be audio- or video-recorded,
A post-prescription waiting period, and
A requirement that the initial evaluation be in person.¹⁶
Residency and Out-of-State Access
Residency requirements vary significantly:
Vermont eliminated its residency requirement in 2023, allowing non-residents to qualify if all statutory criteria are met.⁷
Oregon has also removed its residency requirement.⁸
Many other states, including New York, restrict eligibility to residents only.¹
As a result, Vermont and Oregon may continue to serve as options for some New Yorkers who meet those states’ requirements, particularly before New York’s law takes effect.
Potential Issues Raised by the New Guardrails
Without taking a position for or against the law, advocates and commentators have identified several practical concerns worth noting.
Recorded Oral Requests and Disability Access
The requirement that an oral request be recorded may pose challenges for individuals with speech loss or significant communication impairments, such as those with advanced Parkinson’s disease, stroke-related aphasia, or ALS and other illnesses. Disability-rights advocates have raised concerns that this requirement could unintentionally create barriers for some patients, even when they can communicate clearly through assistive technology.³⁹
Mandatory Mental Health Evaluations
Requiring a psychologist or psychiatrist in every case may result in delays, particularly in rural or underserved areas where mental health professionals are in short supply, even when capacity is otherwise clear.³
Privacy and Documentation
Audio or video recordings of deeply personal medical decisions raise questions about long-term data storage, confidentiality, and access to sensitive records.³
These issues are likely to remain part of the policy conversation as New York moves toward implementation.
Estate Planning Considerations
Medical aid in dying cannot be requested by a health care agent or proxy. The law requires that the request be initiated by the patient themselves.⁴
Accordingly:
A Health Care Proxy cannot authorize medical aid in dying.
A Living Will cannot direct another person to make the request.
That said, estate planning can still play an important role. Some individuals choose to include a non-binding letter of intent—often notarized—expressing their values and wishes regarding end-of-life care. While such a document cannot substitute for statutory requirements, it may provide helpful context and reduce uncertainty for family members and care teams.
What Happens Next
Governor Hochul is expected to sign the law in January 2026, with an effective date six months later.¹ During that time, the Department of Health will develop regulations and guidance for health-care providers.¹
As implementation approaches, continued evaluation and discussion are expected regarding how the law functions in practice.
Conclusion
The Medical Aid in Dying Act represents one of the most significant changes to New York’s end-of-life legal landscape in decades. Its long history, added safeguards, and differences from other states reflect the complexity of balancing patient autonomy, protection of vulnerable individuals, and medical ethics.
For clients engaged in estate planning or administration, the law underscores the importance of clear communication, thoughtful advance planning, and staying informed about evolving legal standards.
Footnotes
Governor Kathy Hochul, Governor Hochul Reaches Agreement with State Legislature to Pass Medical Aid in Dying Act, Dec. 17, 2025, governor.ny.gov.
New York State Senate Bill history, S.138 (initial introductions beginning 2015).
New York Times, “Hochul Agrees to Allow Medical Aid in Dying, With New Safeguards,” Dec. 17, 2025.
New York State Senate, S.138 (2025–2026), Medical Aid in Dying Act, Public Health Law Article 28-F.
CBS News New York, “NY Medical Aid in Dying Bill Explained,” Dec. 2025.
Compassion & Choices; state statutory summaries; CBS News New York, Dec. 2025.
Vermont Department of Health, Patient Choice and Control at End of Life; 2023 statutory amendments removing residency requirement.
Oregon Health Authority, Oregon Death with Dignity Act updates eliminating residency requirement (2023).
Disability-rights commentary and analysis cited in New York Times and regional reporting, Dec. 2025.